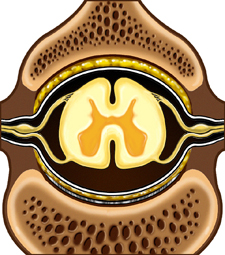
Low back pain is an ache or discomfort in the lower part of the spinal column. It may radiate down into one or both legs. The lower spinal column consists of small, stacked bones (vertebrae) that surround and protect the spinal cord and nerves.
This content was created using EBSCO’s Health Library