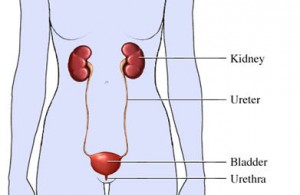
Urinary incontinence is the loss of voluntary bladder control causing leakage of urine. This temporary or chronic condition has multiple mechanisms and many causes. Each cause has its own methods of diagnosis and its own treatment plan.
Urinary bladder function is a careful balance between pressure from the bladder to empty and resistance from the sphincter (valve) at its outlet. Pressure to empty increases suddenly when the bladder reaches a certain volume.
Sphincter resistance depends not only on the strength of the muscle but also on its position. Both forces are controlled mostly by the autonomic (automatic) nervous system, the same system that regulates body temperature, heart rate, blood pressure, digestion, and everything else the body does without thinking about it. We do, however, have muscle control over the sphincter and can strengthen it with exercise.
This content was created using EBSCO’s Health Library