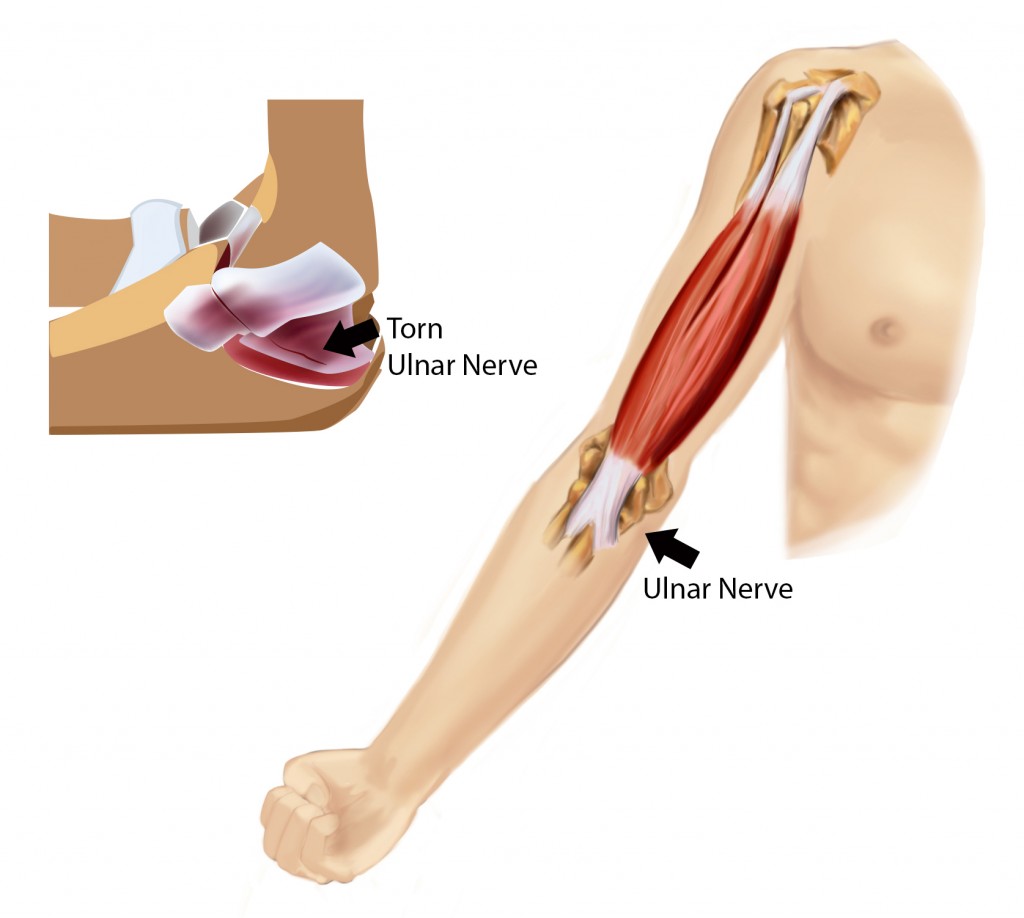
The elbow joint is made of three bones, the long arm bone (humerus) and the two forearm bones (ulna and radius). The elbow joint works like a hinge. The humerus creates the base of the hinge and the olecranon of the ulna rotates nearly 150 degrees around the hinge. The rotation allows for elbow flexion and extension. As the elbow is straightened, the stability of the joint on the inner and outer sections is protected by ligaments that attach bone to bone. The ulnar collateral ligament (UCL) is on the inside of the elbow joint, near the body when the palm is rotated up. It protects the elbow from outward strain that would pull the forearm out of alignment with the humerus.
This content was created using EBSCO’s Health Library