Joint fluid helps the knee move smoothly. A Bakers cyst develops when there is too much of this fluid. The extra joint fluid is pushed out to the back of the knee. Extra fluid may be caused by:
Arthritis—osteoarthritis is the most common type associated with Bakers cysts
Cartilage tears, such as a torn meniscus
Injury or accidents
Infection in joint
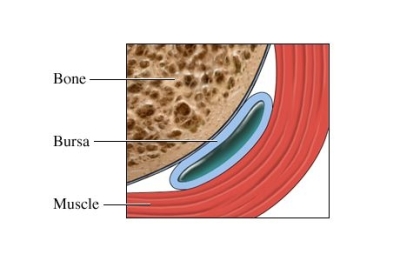
In children, Bakers cyst may be related to a problem with the bursa. The bursa is a small fluid filled sac between the bone and soft tissue.
Factors that increase your risk of Bakers cyst include:
Osteoarthritis
Rheumatoid arthritis
Infectious arthritis
Gout
History of knee injuries or cartilage tears
History of corticosteroid injection around the knee
Previous knee surgery
Knee synovitis
Symptoms may include:
Rounded swelling behind the knee that may get bigger with activity
Pain or pressure in the back of the knee joint—may travel to the calf muscle
Aching or tenderness after exercise and bending the knee
Your doctor will ask about your symptoms and medical history. A physical exam will be done. The doctor will look for a soft mass in the back of the knee. The range of motion in both knees will be tested and compared. The doctor may also shine a special light through the cyst. This will show that the cyst is filled with fluid and not solid.
Images of the knee occasionally needed to look for the cause and extent of the cyst. Images may be taken with:
Ultrasound
CT scan
MRI scan
Blood tests may be taken if there is a possibility of an infection.
Many Bakers cysts resolve on their own without treatment. They usually go away within a two-year period. If a cyst is painful or interferes with daily activities, physical therapy may be helpful to strengthen the muscles around the knee and reduce the swelling.
There is no known way to prevent a Bakers cyst.
This content was created using EBSCO's Health Library
RESOURCES:
National Library of Medicine
http://www.nlm.nih.gov
University Sports Medicine
http://www.ubsportsmed.buffalo.edu
CANADIAN RESOURCES:
Health Canada
http://www.hc-sc.gc.ca
Healthy U
http://www.healthyalberta.com
REFERENCES:
Calmbach WL. Evaluation of patients presenting with knee pain: part II: differential diagnosis. Am Fam Physician. 2003; 68:917-922. Available at: http://www.aafp.org/afp/2003/0901/p917.html.
DynaMed Editorial Team. Popliteal cyst. EBSCO DynaMed website. Available at: https://dynamed.ebscohost.com/about/about-us. Updated November 15, 2011. Accessed January 4, 2013.
Fritschy D, Fasel J, et al. The popliteal cyst. Knee Surg sports Traumatol Arthrosc . 2006;14:623-628.
Torreggiani WC, Al-Ismael K, et al. The imaging spectrum of Baker’s (popliteal) cysts. Clin Radiol . 2002; 57:681-691.
Ward EE, Jacobson JA, et al. Sonographic detection of baker’s cysts: comparison with MR imaging. AJR Am J Roentgenol . 2001: 176:373-380.
This content was created using EBSCO’s Health Library