Post Surgical Rotator Cuff Physical Therapy
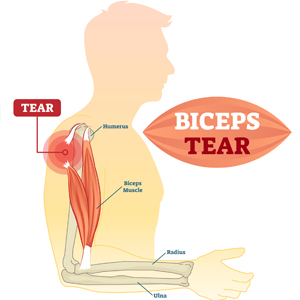
A patient will typically be referred for rotator cuff tear surgery when 90% or more of the tendon is torn. The most common causes for a rotator cuff tear and rotator cuff injuries are aging, overuse of overhead activities and heavy lifting. Surgery should never be taken lightly, so we wanted to take some time to inform you about what to bring before surgery, things that can help you immediately after and then give an idea of what to expect as you go through a post-surgical rotator cuff tear physical therapy treatment plan. These are general guidelines. More specific expectations can be given by your healthcare provider.
Items to bring with you before rotator cuff tear surgery
- Sling
- Ice Pack or Cold Therapy Unit
Using your sling
- You will usually wear it for about 4 weeks. (Removing only to wash up and do exercises)
- Avoid ANY active reaching or lifting up to 6 weeks
- Getting Dressed
– Place the involved arm in the sleeve first.
– Put your belt in your pants first.
– Slip-on shoes are recommended. - Sleeping
– It may be more comfortable sleeping in a recliner instead of a bed.
– Support your arm with a towel roll or pillow if lying down. - Avoid showering for the first couple of days. (Once able to shower, lean over to let your healing arm hang away from your body, while you use the other to wash.)
Icing your shoulder (Ice Pack or Cold Therapy Unit)
- Ice for 20 minutes in your waking hour for the first few days.
- Decrease to 3-5 times a day as needed for pain.
General Care
- Change dressing daily as recommended by your physician/nurse.
- No driving especially if the right arm and if taking pain medications.
- Walk around your home at least 1 time each hour to prevent blood clots.
- Begin therapeutic exercises as soon as instructed
After being cleared for physical therapy, the normal course of a POST-SURGICAL rotator cuff tear physical therapy has been described as having five stages:
Stage 1: Immobilization
There is a mandatory period of rest for the arm following a rotator cuff tear surgery. The tendons have been repaired but need to wait through the biological healing phase in order to be able to accept the strain of moving the arm. This period may last 4-6 weeks and may be intermittent with the therapist being able to do slight motions to the arm to keep the joint from getting stiff.
Stage 2: Passive motion
During and after the immobilization phase, you’ll begin performing passive motion exercises. At first, the therapist will provide the muscle to move the arm, but over time, you’ll be educated in the use of pulleys, stretch straps and table stretches to allow the joint to move while keeping the muscles fully relaxed.
Stage 3: Active-Assisted motion
Once the shoulder has achieved full expected passive motion, and with the permission of the surgeon, your therapist will begin active-assisted motion. This type of exercise uses less than 100% of the surgical shoulder’s power to move the arm. The therapist may instruct you in pendulum exercises that employ gravity and momentum. Self-ranging exercises use the uninvolved arm to move the involved arm, either against the weight of gravity or lying down so that the weight of gravity is minimalized. The surgical arm’s responsibility will slowly increase up to 100% of the weight of the arm. Then, you’ll be ready for active motion.
Stage 4: Active motion
The active motion phase begins when the arm is able to carry its own weight against gravity but is not yet ready to lift, push or pull objects. During this phase, your therapist will demonstrate safe motion patterns of the shoulder and shoulder blade. They will monitor the coordination of movement between the muscles to check for specific weaknesses that could put a strain on the repair. Once you can achieve full expected active range of motion against the weight of gravity, and with your physician’s approval, you’ll be ready to add weight.
Stage 5: Strengthening
The strengthening program may start out slowly. Be patient! The muscles are relearning how to work together so inflammation of the tendons and bursae are still a risk in this phase. Your therapist will recommend exercises that you can do at home in order to improve the arm’s tolerance for strength and to reduce the strain on the arm when you come into therapy. Over time, the therapist will demonstrate ways that you can safely use the arm for pushing up from a chair, pulling a door open, reaching into a cabinet and other activities of daily living.
Post-surgical rotator cuff tear physical therapy care can vary based on the patient’s needs and ability levels. Depending upon the severity of the rotator cuff tear, physical therapy can work with patients to heal the tendon and reduce pain. To find a physical therapist near you click the button below.
![]()